

Recently Diagnosed or Relapsed? Stop Looking For a Miracle Cure, and Use Evidence-Based Therapies To Enhance Your Treatment and Prolong Your Remission
Multiple Myeloma an incurable disease, but I have spent the last 25 years in remission using a blend of conventional oncology and evidence-based nutrition, supplementation, and lifestyle therapies from peer-reviewed studies that your oncologist probably hasn't told you about.
Click the orange button to the right to learn more about what you can start doing today.
- You are here:
- Home »
- Blog »
- Multiple Myeloma »
- Newly Diagnosed Myeloma- Seniors- Darzelex Inc. PFS but Inc. Side Effects!
Newly Diagnosed Myeloma- Seniors- Darzelex Inc. PFS but Inc. Side Effects!


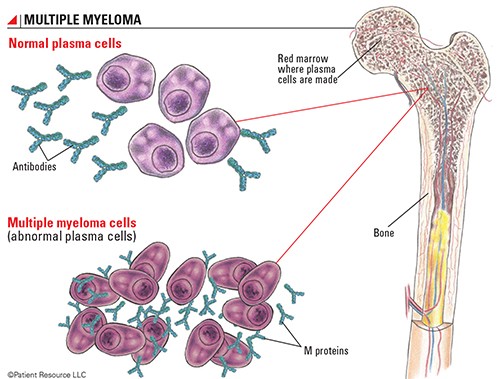
Patients aged 65 years or older with newly diagnosed multiple myeloma, as well as those who have comorbidities, are ineligible for autologous stem cell transplantation.
Adding the chemotherapy called Darzelex makes sense. Adding this chemo to newly diagnosed myeloma patients who are too old for an autologous stem cell transplant (ASCT) can increase your remission (PFS) but it will also increase toxicity aka side effects.
Let me say that again. Adding another chemotherapy (darzalex- daratumumab) to your current chemotherapy regimen for newly diagnosed multiple myeloma may increase your progression-free survival (PFS). But adding a chemotherapy to your regimen will also add toxicity.
Do you want to add toxicity if:
- Your new regimen adds to PFS but not OS (overall survival)? Add length to your remission but not your life?
- Adds toxicity and possibly collateral damage to a newly diagnosed MMer who is transplant-ineligible, older or in poor health?
Please don’t misunderstand me. Achieving complete response and or minimal residual disease-negative status is valuable. But will the added toxicity add quantity to your life? Surely more toxicity will decrease your quality-of-life. Will increase your length-of-life?
Consider evidence-based non-toxic therapies shown to be cytotoxic to MM. Follow an anti-MM diet. Learn about evidence-based anti-MM lifestyle therapies.
I am a long-term MM survivor and MM cancer coach. Watch the free webinar linked on the right of this page and let me know if you have any questions.
Thank you,
David Emerson
- MM Survivor
- MM Cancer Coach
- Director PeopleBeatingCancer
Recommended Reading:
- Language of Oncology- What Multiple Myeloma Patients Need to Know-
- Myeloma Cancer Coaching-Antineoplaston Therapy for Refractory Myeloma
- Myeloma Bone Pain- Cannabinoids, Opioids, Bone Health Therapies?
Addition of daratumumab to chemotherapy doubles PFS in transplant-ineligible newly diagnosed myeloma
“The addition of daratumumab to standard chemotherapy doubled PFS among patients with transplant-ineligible newly diagnosed multiple myeloma, according to late-breaking study results presented at ASH Annual Meeting and Exposition.
Patients who received daratumumab (Darzalex, Janssen) appeared significantly more likely to achieve complete response, and they were more than three times as likely to reach minimal residual disease-negative status…
Patients aged 65 years or older with newly diagnosed multiple myeloma, as well as those who have comorbidities, are ineligible for autologous stem cell transplantation.
A higher percentage of patients assigned daratumumab developed grade 3 or grade 4 infections (23.1% vs. 14.7%), but the percentage of patients who discontinued treatment due to infections was similar between those who received daratumumab-VMP and those who received VMP alone (0.9% vs. 1.4%).
More than one-quarter (27.7%) of patients assigned daratumumab experienced infusion-related reactions. Most (92.7%) occurred during the first infusion, and the majority (95.1%) were grade 1 or grade 2.