

Diagnosed with Cancer? Your two greatest challenges are understanding cancer and understanding possible side effects from chemo and radiation. Knowledge is Power!
Learn about conventional, complementary, and integrative therapies.
Dealing with treatment side effects? Learn about evidence-based therapies to alleviate your symptoms.
Click the orange button to the right to learn more.
- You are here:
- Home »
- Blog »
- side effects ID and prevention »
- Exercise-based Cardiac Rehab- Chemotherapy-induced Cardiomyopathy
Exercise-based Cardiac Rehab- Chemotherapy-induced Cardiomyopathy


“Like medicines, exercise comes with indications and contraindications. And overdosing and under-dosing are both possible.”
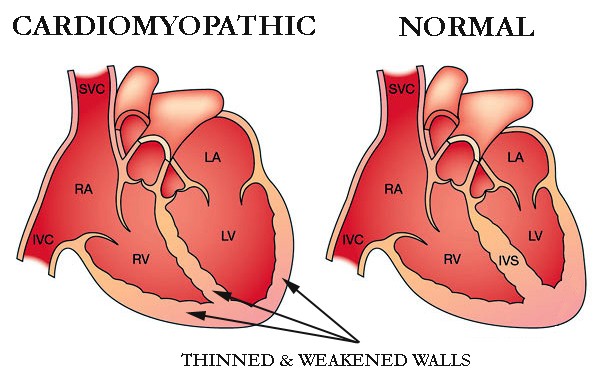
Frequent, moderate exercise is at the heart of both my cancer prevention and cardiac rehab efforts. I am a long-term cancer survivor who was diagnosed with chemotherapy-induced cardiomyopathy (CIC) in late 2010.
Yes, it has occurred to me that I will probably die of conventional oncology treatments, or the side effects caused by those treatments, before I die of my cancer.
However, this combination anger and fear I have toward cancer and oncology helps to drive me to stay healthy. The articles linked and excerpted below describe how I exercise daily.
To be clear, if you saw me working out at my gym, you might think I was “dogging” it. In fact, I’m a bit handicapped (chemo-induced nerve damage…) and my heart doesn’t work too well. So moderation comes easily to me.
But the point of this post is that after several years of research and effort (’15-’20), not only is my cardiomyopathy NOT getting worse, certain metrics are slowly improving! No, I’m not taking any conventional heart medications. No beta blockers, no ACE inhibitors, no nothing…
My experience is that conventional cardiology gives short shrift to evidence-based, non-toxic heart-healthy therapies. Maybe it is only my experience but every cardiology appointment I’ve been has seen my cardiologist aggressively pushing heart meds such as beta blockers, while they briefly mention exercise.
Last month’s Echo showed my ejection-fraction increasing from 40-45 to 50-55. My aortic aneurysm and aortic root have not grown and may also be shrinking (improving). I can’t be sure because of what my cardiologist calls “variation” in my echocardiograms over the past five years.
In any case, I attribute frequent, moderate exercise, heart-healthy nutrition, heart-healthy supplementation and other lifestyle therapies to be the reason why my cardiac rehab efforts are helping me.
Two key points– First, cardiac rehab is about much more than moderate exercise. Conventional medications may well be an important component in your life. I am simply documenting with research and personal experience, that evidence-based but non-conventional heart-healthy therapies can be an essential aspect of your regimen.
Second, there is more to my cardiac rehab efforts than exercise. I have to manage my
- blood pressure,
- my weight,
- my sleep,
- my thinking/attitudes…
- and more.
What I will say is that moderate exercise is one of my non-toxic therapies helping me manage all of these health challenges.
Have you been diagnosed with chemotherapy-induced cardiomyopathy? If you would like to learn more about the evidence-based, non-toxic heart-healthy therapies that I follow daily, weekly, etc. scroll down the page, post a question or comment and I will reply to you ASAP.
Thank you,
David Emerson
- Cancer Survivor
- Cancer Coach
- Director PeopleBeatingCancer
Recommended Reading:
- Heart Failure-Cardiac Rehabilitation & Exercise
- Exercise vs. Drugs to Lower Blood Pressure?
- Heart Failure + Surgery = Higher Risk of Death
Exercise-based cardiac rehabilitation for adults with heart failure.
“Background- Chronic heart failure (HF) is a growing global health challenge. People with HF experience substantial burden that includes low exercise tolerance, poor health-related quality of life (HRQoL), increased risk of mortality and hospital admission, and high healthcare costs.
OBJECTIVES: To determine the effects of exercise-based cardiac rehabilitation on mortality, hospital admission, and health-related quality of life of people with heart failure…
SELECTION CRITERIA: We included randomised controlled trials that compared exercise-based CR interventions with six months’ or longer follow-up versus a no exercise control that could include usual medical care. The study population comprised adults (> 18 years) with evidence of HF – either HFrEF or HFpEF…
MAIN RESULTS:
We included 44 trials (5783 participants with HF) with a median of six months’ follow-up. For this latest update, we identified 11 new trials (N = 1040), in addition to the previously identified 33 trials.
Although the evidence base includes predominantly patients with HFrEF with New York Heart Association classes II and III receiving centre-based exercise-based CR programmes, a growing body of studies include patients with HFpEF and are undertaken in a home-based setting.
All included studies included a no formal exercise training intervention comparator. However, a wide range of comparators were seen across studies that included active intervention (i.e. education, psychological intervention) or usual medical care alone…
CR probably reduces overall hospital admissions in the short term (up to one year of follow-up) and may reduce HF-specific hospitalisation…
After CR, a clinically important improvement in short-term disease-specific health-related quality of life may be evident
Pooling across all studies, regardless of the HRQoL measure used, shows there may be clinically important improvement with exercise
ExCR effects appeared to be consistent different models of ExCR delivery:
- centre vs. home-based,
- exercise dose,
- exercise only vs. comprehensive programmes, and
- aerobic training alone vs aerobic plus resistance programmes.
AUTHORS’ CONCLUSIONS: This updated Cochrane Review provides additional randomised evidence (11 trials) to support the conclusions of the previous version (2014) of this Cochane Review.
Compared to no exercise control,
- CR appears to have no impact on mortality in the short term (< 12 months’ follow-up).
- Low- to moderate-quality evidence shows that CR probably reduces the risk of all-cause hospital admissions and
- may reduce HF-specific hospital admissions in the short term (up to 12 months).
- CR may confer a clinically important improvement in health-related quality of life,
although we remain uncertain about this because the evidence is of low quality. Future ExCR trials need to continue to consider the recruitment of traditionally less represented HF patient groups including older, female, and HFpEF patients, and alternative CR delivery settings including home- and using technology-based programmes.
Too Much Exercise Can Be Harmful, but Moderation Benefits Most
“(Reuters Health) – Exercise, like most things in life, is good in moderation for most people, but extremes can hurt the heart, experts caution in a scientific statement from the American Heart Association…
“Like medicines, exercise comes with indications and contraindications. And overdosing and under-dosing are both possible.”
Kini advises people who are thinking about exercising to choose something they’ll enjoy, whether it’s biking, working out on a treadmill, dancing or Zumba. “It’s got to be something you look forward to,” she said. “And you have to put some effort into weight training as you get older. After age 40 you start losing muscle mass.”
Kerry Stewart, who studies exercise physiology at Johns Hopkins University School of Medicine in Baltimore, said there’s a point beyond which health benefits don’t continue to increase with increasing time spent exercising.
In fact, benefits begin to decline past a certain point, said Stewart, who wasn’t involved in the statement.”