“The relative risk (RR) of heart failure was significantly increased in users of bisphophonates…Similarly, the risk for atrial fibrillation and other arrhythmias as well as heart failure, was significantly higher in patients treated with zoledronic acid compared with in untreated patients…”
The two studies linked and excerpted below offer a sort of circular argument for the MM patient who also take bisphosphonates to strengthen their bones. Many chemotherapy regimens cause heart damage setting up the MM patient for more damage to their heart by bisphosphonate therapy.

Let me explain.
Osteoporosis, osteopenia and bone damage are a common symptom of my cancer, multiple myeloma. Both osteoporosis and osteopenia are a common health problem of the elderly.
Many of the chemotherapy regimens prescribed for patients with multiple myeloma are cardiotoxic and can cause short, long-term and late stage cardiovascular disease aka heart damage.
Cardiovascular disease is common in the elderly and is the number one cause of death in the United Stages today. Cancer is a close number two cause of death.
According to the research linked and excerpted below, the standard-of-care for osteoporosis, osteopenia and bone damage are therapies that can cause cardiovascular disease.
To put this in real terms (at least for me), when I was a newly diagnosed multiple myeloma patient in 1994, I was prescribed high dose bisphosphonate therapy as a part of my standard-of-care MM therapy plan.
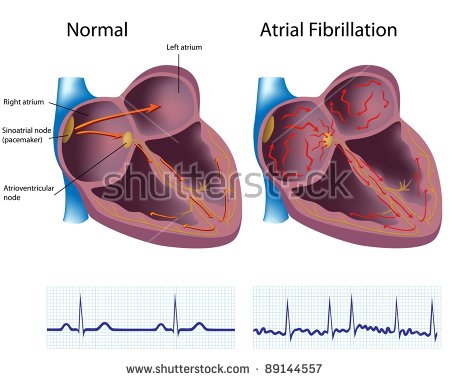
I developed chronic atrial fibrillation (AFib) in late 2010. I was diagnosed with chemotherapy-induced Cardiomyopathy (CIC) shortly thereafter.
I’ll never know if my CIC was caused by the cardiotoxic chemotherapy regimens
- melphalan,
- vincristine,
- busulphan
- cytoxan or
- bisphosphonate therapy.
I underwent all of these therapies. All of these therapies are approved by the FDA as being “safe and effective.” I had an echocardiogram before my autologous stem cell transplant. Dr. Ephron gave me the “all-clear.”
In September of 1997 my oncologist told me that she could do nothing more for me. Two months later I began a non-conventional therapy that is not approved by the FDA. I achieved complete remission from my cancer in early 1999 where I remain today.
I manage my chemotherapy-induced Cardiomyopathy with evidence-based, non-conventional, non-toxic nutrition and supplementation such as CoQ10, C0cao, Taurine, others. These therapies have not been approved by the FDA for safety and efficacy.
If you have been diagnosed with multiple myeloma or have just been diagnosed with osteoporosis or osteopenia, I guess you have to choose between therapies approved by the FDA for safety and efficacy of evidence-based non-conventional, non-toxic therapies.
If you’d like to learn more about non-toxic heart health therapies, scroll down the page, post a question or comment and I will reply to you ASAP.
Hang in there,
David Emerson
- MM Survivor
- MM Cancer Coach
- Director PeopleBeatingCancer
Recommended Reading:
“Results: The mean follow-up times were 2.8, 5.5 and 4.9 years for alendronate-, etidronate- and raloxifene-treated patients, respectively. The absolute risk of heart failure was 4.4% in the exposed group and 3.7% in the control group (P < 0.01).
The relative risk (RR) of heart failure was significantly increased in users of bisphophonates: crude RR 1.71 adjusted hazard ratio (HR) 1.41…
When the two most commonly used bisphosphonates, alendronate and etidronate, were analysed separately, significant trends in the risk of heart failure were observed across refill compliance strata.
The risk of heart failure increased significantly with increasing refill compliance for etidronate, whereas it decreased for alendronate.
Conclusions: Bisphosphonate users were at increased risk of heart failure compared to age- and gender-matched control subjects. However, users of alendronate showed a dose-dependent reduction in this risk, suggesting that alendronate may reduce the risk of heart failure.
“Patients treated with zoledronic acid had a higher risk for heart failure, among other cardiovascular conditions, according to a study presented at the American Society for Bone and Mineral Research (ASBMR) 2017 Annual Meeting held September 8-11 in Denver, Colorado.1
Researchers from the University of Southern Denmark in Odense analyzed data from a 5-year propensity score matched cohort from 2 national health registries to determine the incidence of safety-related outcomes in patients treated with zoledronic acid (21,520 person-years) vs patients treated with oral bisphosphonates (63,020 person-years) or untreated patients (63,880 person-years).
During a median period of 2.4 years, the researchers observed a higher risk for heart failure in patients treated with zoledronic acid compared with patients treated with oral bisphosphonates.
Similarly, the risk for atrial fibrillation and other arrhythmias as well as heart failure, was significantly higher in patients treated with zoledronic acid compared with in untreated patients…
The researchers could not definitively conclude that the higher rates of cardiovascular events were related to a drug effect, a difference in risk at baseline, or both, because of the study’s observational nature.
“It is possible that [zoledronic acid] was targeted to a frailer subset of patients than [oral bisphosphonates],” they wrote. “[Al]though propensity score matching and confounder adjustment was employed to reduce the influence of confounding, information on confounders such as smoking, alcohol, exercise, and [body mass index] is not available in national registries.”
“On 13 May 2013, Servier released a Direct Healthcare Professional Communication which stated that new restrictions for the use of strontium ranelate are now in place, as randomised trials have shown an increased risk of myocardial infarction…
…The European Pharmacovigilance Risk Assessment Committee (PRAC) recommends restriction in the use of strontium ranelate, based on a routine benefit-risk assessment of the medicine, which included data showing an increased risk of heart problems, including heart attacks.[3]
On 21 February 2014 the European Medicine Agency recommended that strontium ranelate remain available with restrictions relative to patients with existing heart disease.[4]”
“Background: In a globally aging population, chronic conditions with a high impact on healthcare costs and quality of life, such as osteoporosis and associated fractures, are a matter of concern.
For osteoporosis, several drug treatments are available, but evidence on adverse cardiovascular and cerebrovascular (CCV) events, and in particular the risk of atrial fibrillation (AF), related to anti-osteoporotic drug use is inconclusive.
The objective of this study was to evaluate the association between the use of bisphosphonates (BPs), strontium ranelate (SR), and other anti-osteoporosis drugs and the risk of AF and CCV events in a large cohort of patients affected by CCV diseases…
Results: The initial cohort accounted for 657,246 patients. Neither BPs nor SR use was associated with an increased risk of AF regardless of the adherence and recency of use.
Overall BP and SR use was associated with a slightly increased risk of CCV; however, results reversed when considering higher adherence…
Conclusions: BPs do not increase cardiovascular risk and can be prescribed to elderly patients for osteoporosis treatment. However, patients with pre-existing cerebrovascular/cardiovascular conditions should be carefully monitored.
Hip Fracture, Osteoporosis- Bisphosphonate Therapy?
Bisphosphonate therapy side effects include- Upset Stomach/Esophageal Inflammation, Osteonecrosis of the Jaw, Bone, Joint, and Muscle Pain, Femur Fracture
Hi David- I’ve been following PeopleBeatingCancer for the past year or so. My husband has been battling multiple myeloma for 5 years so I am always looking for ways to help him. However I have just been diagnosed with osteoporosis after I broke my right humerus and left wrist when I fell.
My doctor wants me to have an infusion of bisphosphonate therapy.
Do you think I could strengthen my bones without this? I’m not happy about receiving this drug after reading about side effects. I am 73 and fairly active.
Hi Rose-
Osteoporosis is common in both MM patients as well as people over 70. Regarding your question “Do you think I could strengthen my bones without this? I’m not happy about receiving this drug after reading about side effects” the simple answer is yes.
I will add the MM CC program bone health guide below. Both you and your husband can take any of the nutritional supplements and pursue lifestyle therapies shown to build bone health and enhance your bone mineral density aka bone strength.
The longer and more complete answer is that the reason why medical doctors prescribe bisphosphonate therapy (boniva in pills, aredia intravenously, many others) is because drug companies have to go through the FDA approval process to get FDA approval. FDA approval is required for health insurance and Medicare to pay for a therapy. This is how medicine works in our country.
Some doctors will talk about nutritional supplementation such as calcium and vitamin D3. You should probably supplement with those two regardless. But those two bone therapies have not been tested, nor approved by the FDA.
The side effects associated with bisphosphonate therapy, osteonecrosis of the jaw/ONJ, is usually associated with long-term bisphosphonate use. Studies show that the majority of the bone hardening benefit of bisphophonate therapy results in the first few months of use.
My point is that if your bones are really weak and you are worried about another fall, you could undergo a month or two of bisphophonate therapy, stop the continue with non-toxic bone health therapies all outlined in the bone health guide below.
My apologies for my longwinded answer. Let me know if you have any questions. Please, please, please rehabilitate your hip and wrist.
Hang in there,
David Emerson
- MM Survivor
- MM Coach
- Director PeopleBeatingCancer
Recommended Reading:
“Bisphosphonate medications have become a
common treatment for patients with
osteoporosis. Bisphosphonate medications have been found to increase bone strength and lead to a lower chance of fracture in the first 5 years after starting the medication. Many patients have been prescribed a bisphosphonate medication (such as Fosamax, Boniva, or Actonel), and these patients should be aware of possible side effects of these drugs…
Upset Stomach/Esophageal Inflammation
The most common side effect of bisphosphonate medications is stomach upset. The medication can cause inflammation of the esophagus and even lead to erosions of the surface of the esophagus…
Osteonecrosis of the Jaw
…This complication typically occurs in people taking IV doses of bisphosphonates, and is usually seen after a patient on bisphosphonate medication has had dental surgery involving the jaw.
Bone, Joint, and Muscle Pain
This complication may arise days, months, or even years after starting bisphosphonate therapy. If severe muscle or bone pain is a problem, stopping bisphosphonate medication should be considered. Speak to your doctor about your symptoms.
Femur Fracture
Unusual femur fractures have been found in some patients taking bisphosphonate medications for lengthy time periods…”
“With bisphosphonates, however, the antiresorptive effect is maintained because these agents “adhere very strongly to bone surfaces and therefore… remain in the bone for years after stopping taking the drug,” according to a review published in the European Journal of Endocrinology.1
For this reason, it has been proposed that some patients may benefit from periodic breaks from bisphosphonates, also referred to as drug holidays, to reduce unnecessary treatment along with the risk for adverse effects…”