

Recently Diagnosed or Relapsed? Stop Looking For a Miracle Cure, and Use Evidence-Based Therapies To Enhance Your Treatment and Prolong Your Remission
Multiple Myeloma an incurable disease, but I have spent the last 25 years in remission using a blend of conventional oncology and evidence-based nutrition, supplementation, and lifestyle therapies from peer-reviewed studies that your oncologist probably hasn't told you about.
Click the orange button to the right to learn more about what you can start doing today.
- You are here:
- Home »
- Blog »
- Multiple Myeloma »
- Myeloma – Anthracycline – Cardiomyopathy –
Myeloma – Anthracycline – Cardiomyopathy –


The incidence of late progressive (anthracycline-induced cardiomyopathy) cardiovascular disease in long-term survivors of cancer is established and may contribute to heart failure and death.
In 2010 I was diagnosed with antracycline-induced cardiomyopathy. The first study linked and excerpted below is dated 2007 states that people like me “have not been systematically studied.”
The study below that one is from 2006 and says that “Cardiac damage has been shown at cumulative doses as low as 200 mg/m2, well below levels currently assumed to induce injury.”
Finally, the study from the year 2000 states that “Twenty seven to sixty percent of patients with anthracycline-induced cardiomyopathy die of congestive cardiac failure.”
I don’t like to question conventional oncology but I don’t think oncology has much understanding of the long-term effects of chemotherapy. Certainly not anthracycline-induced cardiotoxicity.
To be fair, my Cardiomyopathy might not have occurred only because of VAD, Dr. Berger also prescribed:
- melphalan,
- busulphan
- cytoxan and
- bisphosphonate therapy.
all of which are cardiotoxic, all cause damage to the heart. In addition, Dr. Barry Ephron gave me the thumbs up after and echo, so I can’t blame it all on Dr. Berger…
Which brings me to the real issue of this post. Adverse events better known as side effects. More specifically:
- Short-term,
- Long-term and
- Late stage side effects.
Short term side effects such as your hair falling out (alopecia), nausea, fatigue, etc. are all examples of short-term side effects that usually resolve in the days or weeks once you discontinue chemo or radiation.
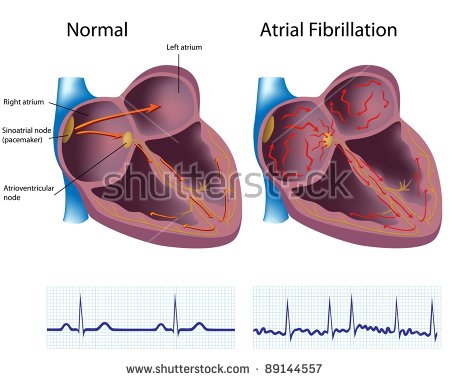
In this case, I am talking about late stage side effects. The idea that one day in the fall of 2010, I flipped into chronic atrial fibrillation (AFib), went to a cardiologist who then confirmed, yes, it was my high-dose, aggressive chemotherapy regimens from 1995, that caused my heart damage.
To quote the research below:
- “which are progressive and irreversible from the first dose.”
- “anthracycline cardiotoxicity is associated with slowly progressive deterioration of cardiac function, which continues for years after treatment cessation.”
My point is that my oncologist gave me several chemotherapy regimens that was almost guaranteed to cause Cardiomyopathy eventually. I’m not dead yet but, according to the studies below, I have a 27%-60% chance of dying from cardiovascular disease.
Enough of my whining… So what can be done about my chemotherapy-induced Cardiomyopathy?
The same cardiologist who diagnosed me in late 2010 prescribed a drug called metoprolol. I tried it and immediately experienced severe shortness of breath.
According to my research, there are a series of evidence-based but non-toxic therapies that should help my heart health.
- Exercise
- Nutrition
- Supplementation (CoQ10, cacao, DHEA, others)
- Sauna
And the list goes on. And many of these therapies help my anti-cancer lifestyle as well.
A person living with chemotherapy-induced Cardiomyopathy may want to pursue a complementary approach to his/her heart health. That is to say he/she would combine conventional therapies with evidence-based non-conventional therapies. While cardiology often talks about the importance of exercise, diet, etc. I have never heard any of my cardiologists mention a word about exercise, diet or nutritional supplementation.
I guess the point of all this is that long-term cancer survivors face a high and ever increasing risk of a host of different side effects. Completing chemotherapy and growing your hair back isn’t the end of it.
Regular check-ups aren’t the solution to long term adverse events either. My heart function was fine for 15 years post chemo and then one day…bam! I don’t think a GP would have seen that one coming. I should have started my heart health regimen years before I did.
To Learn More about Chemotherapy-induced Heart Damage- click now
To learn more about evidence-based, non-toxic, non-conventional heart therapies scroll down the page, post a question or comment and I will reply to you ASAP.
Thank you,
David Emerson
- MM Survivor
- MM Cancer Coach
- Director PeopleBeatingCancer
Recommended Reading:
- Multiple Myeloma Survivors, Cardiovascular Disease and How to Treat It
- Multiple Myeloma Side Effects- CoQ10 Prevents Chemo Cardiotoxicity
Anthracycline-induced cardiotoxicity: course, pathophysiology, prevention and management.
2007 Jun;
Although effective anti-neoplastic agents, anthracyclines are limited by their well recognized and pervasive cardiotoxic effects. The incidence of late progressive cardiovascular disease in long-term survivors of cancer is established and may contribute to heart failure and death.
To maximize the benefits of these drugs, a high-risk population has been identified and new strategies have been investigated to minimize toxic effects, including limiting the cumulative dose, controlling the rate of administration and using liposomal preparations and novel anthracycline analogues. Dexrazoxane also shows promise as a cardioprotectant during treatment.
This paper reviews these strategies, as well as medications used to manage anthracycline-induced cardiotoxicity, and functional and biochemical means of monitoring cardiotoxicity, including echocardiography, radionuclide scans and biomarker analysis.
The treatment of adult cancer survivors who have had anthracycline-related cardiotoxicity has not been systematically studied.
Empirically, anthracycline-associated cardiac dysfunction is treated very similarly to other forms of heart failure. These treatments include avoiding additional cardiotoxic regimens, controlling hypertension, lifestyle changes, medications and heart transplantation.
Pathogenesis of cardiotoxicity induced by anthracyclines.
2006 Jun;
“Anthracyclines are potent anti-neoplastic drugs used in the treatment of solid and hematologic cancers. However, their use is limited by cumulative dose-related cardiotoxic adverse effects, which are progressive and irreversible from the first dose.
Clinical trial data have shown that anthracycline cardiotoxicity is associated with slowly progressive deterioration of cardiac function, which continues for years after treatment cessation.
Cardiac damage has been shown at cumulative doses as low as 200 mg/m2, well below levels currently assumed to induce injury. The widespread use of anthracyclines in childhood leukemia has resulted in an improved long-term prognosis; however, these patients are subsequently at high risk of developing long-term cardiac damage, with studies suggesting as many as 65% of survivors of childhood leukemia will develop cardiac abnormalities.
Middle aged and elderly patients who are prone to cardiac disease may be more vulnerable to the cardiotoxic effects of anthracyclines.
Therapies or strategies to prevent anthracycline-inducedcardiotoxicity are essential; ideally, these should be initiated at the beginning of anthracycline therapy to reduce the possibility of cardiac damage and to ensure the optimal use of chemotherapy…”
[Cardiotoxicity of anthracycline].
2000;54
“The anthracyclines are among the most active and useful anticancer agents, but they are also the most common chemotherapeutics associated with the development of congestive heart failure.
Twenty seven to sixty percent of patients with anthracycline-induced cardiomyopathy die of congestive cardiac failure. The paper presents the pathomechanisms of anthracycline-induced cardiotoxicity and perspectives on prevention of congestive heart failure resulting from anthracycline chemo-therapy…”