

Recently Diagnosed or Relapsed? Stop Looking For a Miracle Cure, and Use Evidence-Based Therapies To Enhance Your Treatment and Prolong Your Remission
Multiple Myeloma an incurable disease, but I have spent the last 25 years in remission using a blend of conventional oncology and evidence-based nutrition, supplementation, and lifestyle therapies from peer-reviewed studies that your oncologist probably hasn't told you about.
Click the orange button to the right to learn more about what you can start doing today.
- You are here:
- Home »
- Blog »
- Multiple Myeloma »
- Multiple Myeloma Bone Lesions- Decreased BMD = Mortality
Multiple Myeloma Bone Lesions- Decreased BMD = Mortality


“ elderly patients who suffer an osteoporosis-related hip fracture have an increased 1-year mortality of 12–37%.2“
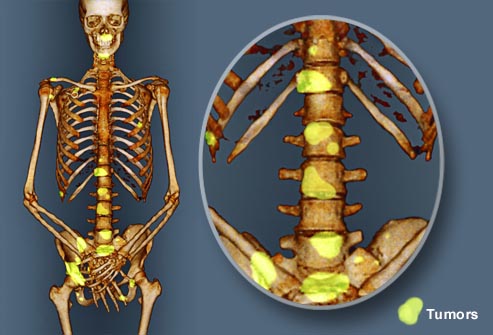
Multiple myeloma is a blood cancer and bone disease at the same time. I say this because according to research, 80%-90% of MM survivors develop pathological fractures and/or lytic lesions. Enhancing bone mineral density (BMD) is a lifelong process for MM survivors. Unfortunately, not only does the MM disease itself damage BMD, but standard-of-care therapies decrease BMD as well.
According to the research linked and excerpted below:
- Autologous Stem Cell Transplant can decrease bone mineral density
- Dexamethasone can decrease bone mineral density
Like kidney damage, blood clots, and anemia, decreased bone mineral density and the bone damage that can result, is both a multiple myeloma symptom and a side effect of MM therapy.
So what is the newly diagnosed multiple myeloma patient or survivor to do? No, I am not advocating that you not undergo dexamethasone or other chemotherapy regimens that may weaken your bones.

I am advocating that you take a “less is more” approach to conventional standard-of-care (SOC), FDA approved therapies.
For example, if you are considering an autologous stem cell transplant, the long-term bone damage caused by ASCT discussed below, may be yet another strike against this SOC, FDA approved MM therapy.
Further, if you one of the fortunate 30%-40% who reach either MRD or CR after 3-4 cycles of their induction therapy, consider discontinuing more chemotherapy for the time being now that you know that the more toxic chemotherapy you undergo the more short, long-term and late stage side effects you may incur.
Finally, consider undergoing those evidence-based but non-toxic therapies shown to enhance bone mineral density such as:
- nutritional supplementation (vitamin D3, curcumin, magnesium, etc.)
- bone building nutrition
- bone building lifestyle therapies
The payoff is these above mentioned therapies are inexpensive, are anti-MM and therefore may reduce your risk of MM relapse and they all will strengthen your immune system and speed your post-induction healing process.
The long-term damage done to MM survivors’ bones, bone marrow, kidney, heart, brain, eyes, etc. is not well understood by medical science. I have been researching my cancer (MM) for more than 15 years now and it has taken me all these years to uncover the research that is documenting the dramatic damage done by toxic SOC therapies.
Please understand that conventional oncology and the FDA are not in the business of studying the long-term and late stage side effects that can result from toxic chemotherapy and radiation. This is not what they do.
I believe that it is up to the MM patient, survivor and caregiver to understand the positives and negatives of their SOC MM therapies and act accordingly.
If you would like to learn more about the long-term damage done to the MM patient/survivor and learn how to manage yourself, scroll down the page, post a question or comment and I will reply to you ASAP.
In the meantime, good luck and hang in there.
Thank you,
David Emerson
- MM Survivor
- MM Coach
- Director PeopleBeatingCancer
Recommended Reading:
- Multiple Myeloma Therapy- Healing Lytic Lesions
- Multiple Myeloma Therapy, Magnesium, Bone Mineral Density
- Healing Bone Loss in the Multiple Myeloma Survivor
Fracture risk for MM patients remains higher despite improvements in treatments, survival
“Bone lesions are one of the primary symptoms in multiple myeloma (MM), and approximately 80% of patients experience a pathological fracture at initial presentation or during the course of the disease…
Their retrospective case-control study included 1,334 patients with MM in Denmark from the Danish National Health Service, of which 881 sustained a fracture between 1996 and 2011. MM patients were matched to patients from the database without MM…
The researchers found that the risk of any fracture was significantly higher in MM patients, compared with patients without MM at all three time periods examined, and remained high over time…
“New treatment strategies, even if they have a positive impact on overall survival, offer no guarantee for a corresponding reduction in bone lesions,” the authors concluded…”
Decreased bone mineral density is common after autologous blood or marrow transplantation
“Survivors of autologous blood or marrow transplantation (ABMT) are predisposed to decreased bone mineral density (BMD), but data are lacking on the incidence and risk factors for this condition…
As the number of long-term survivors of autologous blood or marrow transplantation (ABMT) increases, greater attention is turning to the late complications of this procedure. One such complication is decreased bone mineral density – osteopenia and osteoporosis…
In the short term, osteoporosis seems trivial compared with a diagnosis of cancer, but for those cured of their disease, decreased bone mineral density contributes to chronic morbidity and mortality in the form of bone fractures. For example, 50% of patients who sustain an osteoporosis-related hip fracture require assistance with activities of daily living1 and elderly patients who suffer an osteoporosis-related hip fracture have an increased 1-year mortality of 12–37%.2
Decreased BMD can lead to significantly increased morbidity and mortality because of osteoporosis-related bone fractures…”
Dexamethasone treatment impairs calcium regulation and reduces bone mineralization in infant pigs.
“Calcium and vitamin D metabolism, bone mineralization, and growth were studied in piglets randomly assigned to 15 d of dexamethasone (0.5 mg.kg-1.d-1, orally) or placebo. Growth velocity was significantly reduced by dexamethasone treatment (P < 0.001).
Pigs in the dexamethasone group demonstrated lower 45Ca absorption by in situ intestinal perfusion (P < 0.01). Plasma 25-hydroxycholecalciferol (calcidiol) and 1,25-dihydroxycholecalciferol (calcitriol) were lower (P < 0.05) and the urinary ratio of calcium to creatinine was higher (P < 0.05) after 15 d of dexamethasone compared with placebo.
Differences between pre- and postosteocalcin were higher and whole body, lumbar, and femur bone mineral density were lower in dexamethasone-treated piglets.
Dexamethasone-induced reductions in bone mineral mass likely result from reduced vitamin D status, reduced intestinal calcium absorption, elevated urinary calcium loss and direct effects of the steroid on bone.
When dexamethasone is used in premature infants to improve lung function, negative effects on growth and bone metabolism could occur.”