

Recently Diagnosed or Relapsed? Stop Looking For a Miracle Cure, and Use Evidence-Based Therapies To Enhance Your Treatment and Prolong Your Remission
Multiple Myeloma an incurable disease, but I have spent the last 25 years in remission using a blend of conventional oncology and evidence-based nutrition, supplementation, and lifestyle therapies from peer-reviewed studies that your oncologist probably hasn't told you about.
Click the orange button to the right to learn more about what you can start doing today.
- You are here:
- Home »
- Blog »
- Multiple Myeloma »
- Multiple Myeloma Side Effects- VTE, Blood Clot Risk Reduction
Multiple Myeloma Side Effects- VTE, Blood Clot Risk Reduction


“With an aging population and a rising prevalence of obesity and cancer (MM), the incidence of VTE is expected to increase in the coming years…”
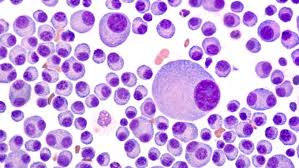
If you’ve been diagnosed with multiple myeloma (MM), your risk of a blood clot (DVT/VTE) will increase. If you undergo chemotherapy, the risk of this common MM side effect, will increase significantly.
According to the article linked below, if you are about 67 (average age of MM patients) and overweight, your risk of blood clot increases even more.
While you can always just take a pill to reduce your risk of VTE somewhat, increasing “cardiorespiratory fitness” levels will reduce your risk of VTE without the side effects of oral coagulants. Further, frequent, moderate exercise complements your chemo, strengthens your bones and reduced your risk of multiple myeloma relapse.
In short, frequent, moderate exercise is just about the most effective, least expensive, easiest therapy that you will ever do…ever.
I’m not trying to condem standard-of-care FDA approved therapies. I’m trying to offer evidence-based, non-toxic therapies that can either reduce or replace your need for conventional therapies that may very well cause as many side effects as health problems that they address.

Moderate exercise, omega-3 fatty acids, curcumin and others have all been shown to enhance chemotherapy, reduce the risk of VTE (blood clots), while they fight multiple myeloma itself.
I was diagnosed with MM in early 1994. Shortly after starting my induction chemo I developed a VTE. My oncologist said nothing about non-toxic therapies before or after my blood clot struggles. Dr. Berger simply put me in the hospital for a few days and prescribed intravenous heprin.
Which was the standard-of-care for VTE’s at the time. Because I developed another VTE in the other leg two years later, I wish Dr. Berger had talked to me about non-toxic therapies to reduce my risk of blood clots.
If I knew then what I know now…
Have you been diagnosed with MM? Have you developed a VTE? Are you hoping to prevent a venous thromboembolism? Scroll down the page, post a question or comment and I will reply to you ASAP.
Hang in there,
David Emerson
- MM Survivor
- MM Cancer Coach
- Director PeopleBeatingCancer
Recommended Reading-
- Integrative Approaches, Lifestyle Therapy Enhance Multiple Myeloma survivorship.”
- The Cure for Multiple Myeloma? Exercise
- Multiple Myeloma- Tally DVT/VTE Risk Before Revlimid, Thal, Pom, Imnovid
Greater cardiorespiratory fitness may reduce risk for venous thromboembolism
“Higher estimated cardiorespiratory fitness levels appeared associated with a lower risk for venous thromboembolism, according to results of a population-based cohort study published in Journal of Thrombosis and Haemostasis.
Researchers observed the correlation independent of weight status, which suggests a higher estimated cardiorespiratory fitness level may attenuate the association between obesity and VTE.
“With an aging population and a rising prevalence of obesity and cancer (MM), the incidence of VTE is expected to increase in the coming years,” Line H. Evensen, MSc,PhD fellow in the department of clinical medicine at The Arctic University of Norway, and colleagues wrote. “Identification of modifiable risk factors at the population level is currently a priority to curb the growing burden of VTE.”
Growing evidence has linked physical activity to a lower risk for VTE; however, that evidence is controversial because of inconsistent definitions of physical activity, the variety of measuring instruments available and a reliance on self-reported data…
Cardiorespiratory fitness was estimated based on sex-specific algorithms that accounted for age, waist circumference, resting heart rate and self-reported physical activity.
Mean estimated cardiorespiratory fitness was 31.5 ± 5.7 mL/kg/min among women and 38.8 ± 6.8 mL/kg/min among men.
Results showed that after 83,729 person-years of follow-up (median duration, 8.5 years; interquartile range, 8.2-8.9), 176 VTE events occurred, for a crude incidence rate of 2.1 (95% CI, 1.8-2.4) per 1,000 person years.
Median age at the time of incident VTE was 69 years, and 55.1% of all events occurred among men.
Pulmonary embolism with or without concomitant deep vein thrombosis accounted for 56.3% of all events, with the remainder (43.7%) being isolated incidences of DVT.
Additionally, cancer played a provoking role in 30.7% of the VTE events.
Compared with individuals who had estimated cardiorespiratory fitness less than 85% of age-predicted level, those with cardiorespiratory fitness of 85% to 100% of age-predicted level had a 46% (HR = 0.54; 95% CI, 0.39-0.77) lower risk for VTE, whereas those with more than 100% of age-predicted cardiorespiratory fitness had a 67% (HR = 0.33; 95% CI, 0.2-0.54) lower risk.”