

Diagnosed with SMM, SPB, or MGUS?
Learn how you can stall the development of full-blown Multiple Myeloma with evidence-based nutritional and supplementation therapies.
Click the orange button to the right to learn more.
- You are here:
- Home »
- Blog »
- Pre-Myeloma »
- Smoldering Becoming Multiple Myeloma?
Smoldering Becoming Multiple Myeloma?


“The good news is that, according to research, your nutritional supplementation and diet are “prehabilitating” you. By this I mean that, on average, you should respond to the induction therapy that your oncologist is recommending.”
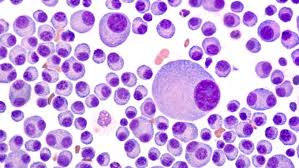
Hi David. I am 53 year old, Asian man living in US. I have been a Smoldering Multiple Myeloma patient for two years. My oncologist is telling me that I have graduated to a multiple myeloma diagnosis. During two years, I’ve taken nutritional supplements such as-
- Curcumin(8g/day),
- Vitamin-C,
- selenium,
- Green tea extract (1000mg/day),
- Inositol(1000mg/day),
- IP6,
- Ashwagandha,
- black-seed oil,
- Omega-3 Fatty Acids,
- CBD oil,
- wheat grass extract powder.
My main diet is with the cooked rice, some vegetables, some meat not daily.
But the blood test on March-10-2020 shows-
- Free K/L ratio is 161 (Kappa light chain=500(mg/L), lambda light chain=3.1(mg/L)).
- Also M-spike (SPE, g/dL) = 5.4
The ratio and M-spike is increasing last 6 months. My latest WBC=5.9(K/uL), RBC=3.52(M/uL), HGB=11.7(g/dL), PLT=236(K/uL), Albumin=2.2(g/dL), Globulin=9.7(g/dL), BUN=16(mg/dL), Creatine=1.1(mg/dL), Calcium=8.4(mg/dL).

So my oncologist suggested me to start the treatment with Revlimid + Velcade + Dexamethasone. I am also going to have PETscan, biopsy next week.
Currently I feel anemia. I think this feeling has been last two weeks. Previously I thought my supplement maintains well smoldering. But it seems like not. Maybe my recent added CBD oil (taking one month) might not work well with me.
Would you give me some advice based on my current condition? Thank you. Chan
Dear Chan,
I should see a complete set of your blood urine and imaging testing but if I understand your current stage, your SMM as become early stage MM. Your fatigue aka anemia is probably a result of low red blood cells taking up reduced amounts of oxygen.
The good news is that, according to research, your nutritional supplementation and diet are “prehabilitating” you. Several of the nutritional supplements you have been taking have been shown to by cytotoxic (kill) MM cells. Prehabilition with these supplements means that, on average, you should respond to the induction therapy that your oncologist is recommending. You should experience fewer side effects too.
Being a young man (the average MM patient is 69 years old), I believe you should focus on your long-term goals meaning the 10, 20,30 year picture. I think that prehabilitation followed by modest amounts of toxicity (less than what the average oncologist will promote) accompanied by evidence-based, non-toxic therapies such as your nutritional supplementation, frequent exercise, nutrition, detox, etc. is your best chance of reaching those goals.
If you are interested I am happy to assess your PET scan results as well as your bone marrow biopsy results as well. Your call. No charge, just informational.
Good luck- let me know if you have any other questions.
David Emerson
- MM Survivor
- MM Coach
- Director PeopleBeatingCancer
Recommended Reading:
Cancer prehabilitation: One step toward improved outcomes
“The future of high-quality cancer treatment will increasingly focus on patient-centered care, supported by a strong evidence base and highly skilled providers. Nurses, particularly navigators, are uniquely positioned to deliver efficacious prehabilitation services. With this unique opportunity comes the responsibility to understand the evidence-based research and incorporate it into a best practices clinical approach to improving cancer care. Because research in this area of medicine is rapidly evolving, nurses should consider pursuing formal training and continuing education in cancer prehabilitation and collaborate more closely with rehabilitation health care professionals…”
Curcumin induces cell death of the main molecular myeloma subtypes, particularly the poor prognosis subgroups.
“Multiple myeloma (MM), a plasma cell malignancy, remains incurable despite the development of new therapies. Curcumin anti-tumor effects were previously characterized in multiple myeloma, however only few MM cell lines were included in these studies.
Since myeloma is a heterogeneous disease it is important to address the impact of myeloma molecular heterogeneity in curcumin cell death induction.
In the present study, a large panel of human myeloma cell lines (HMCLs) (n = 29), representing the main molecular MM subgroups, was screened for curcumin sensitivity. We observed that curcumin cell death induction was heterogeneous, of note 16 HMCLs were highly sensitive to curcumin (LD50 < 20.5 μM), 6 HMCLs exhibited intermediate LD50 values (20.5 μM ≤ LD50 < 32.2 μM) and only 7 HMCLs were weakly sensitive (35 < LD50 < 56 μM).
Cell lines harboring the t(11;14) translocation were less sensitive (median LD50 32.9 μM) than non-t(11;14) (median LD50 17.9 μM), which included poor prognosis t(4;14) and t(14;16) cells.
Interestingly, curcumin sensitivity was not dependent on TP53 status. For the first time we showed that primary myeloma cells were also sensitive, even those displaying del(17p), another poor prognosis factor…
Altogether, these results support clinical trials including curcumin in association with standard therapy.”
EPA and DHA have selective toxicity for PBMCs from multiple myeloma patients in a partly caspase-dependent manner
“Poly-unsaturated fatty acids (PUFAs) have been shown to have cytotoxic effects in both solid and non-solid tumors. Eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA) are among the most studied PUFAs.
The aim of the present study was to evaluate the cytotoxic effects of these two fatty acids (FAs) in the peripheral blood mononuclear cells (PBMCs) obtained from untreated patients (new cases) with confirmed symptomatic multiple myeloma (MM).
Our results showed that EPA at the concentration of 100 μM and DHA at 50 and 100 μM induce potent apoptotic effects in the PBMCs of MM patients (P < 0.05) as evidenced by Annexin V and propidium iodide (PI) staining, while they have little or no effects on the PBMCs isolated from healthy donors (P > 0.05).
The observed effects were concentration- and time-dependent…
The results of the present study showed that EPA and DHA have selective toxicities for malignant human plasma cells from MM patients, but not for mononuclear cells of healthy donors. These results warrant further studies with larger study populations to investigate the usefulness of PUFAs as a promising adjunctive therapy in the treatment of MM…”