
- You are here:
- Home »
- Blog »
- non-conventional therapies »
- Incurable HPV-Related Cancer- Oropharyngeal, Cervical, Anal-
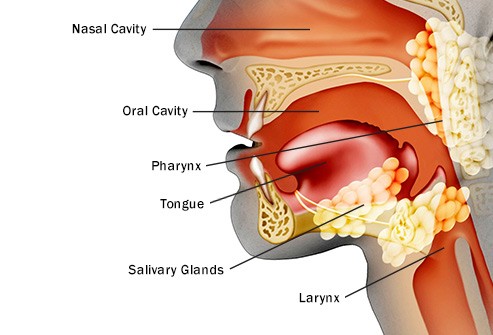
Incurable HPV-Related Cancer- Oropharyngeal, Cervical, Anal-


The analysis included 24 patients (median age, 60 years; men, n = 20) with incurable HPV-16-related cancers (oropharyngeal, n = 22; cervical, n = 1; anal, n = 1).
The good news is that the therapies Nivolomab and HPV vaccine have never been combined before for the treatment of incurable HPV related oropharyngeal (head and neck), cervical and anal cancers…and a bit more than a third of the patients in the study responded. The not-so-good news is that the study was small, 24 patients, and the response was limited.
I was also told that my cancer was incurable…in 1994. My point is that conventional oncology can be…limited. I found that being told I was end-stage pushed me to think outside-the-box.
HPV is also a risk factor for my cancer. Conventional oncology considers my cancer to be incurable. Upon diagnosis, I later found out that I had the HPV virus. I have since learned that the non-toxic supplement AHCC treats HPV. The brand of AHCC that I took is Now Brand.
To further the concept of integrating conventional and non-conventional therapies, studies show that immnotherapy can be enhanced with probiotics.
My point is that if you have been told your cancer or stage of cancer is incurable, then it may be time to think outside-the-box. Consider evidence-based but non-conventional aka therapies not discussed by your oncologist, therapies such as
- nutrition,
- supplementation (probiotics),
- and lifestyle therapies.
Have you been diagnosed with incurable cancer? Would you like some help thinking outside-the-box? Scroll down the page, post a question or comment and I will reply to you ASAP.
Thank you,
David Emerson
- Cancer Survivor
- Cancer Coach
- Director PeopleBeatingCancer
Recommended Reading:
Cancer, Mind-Body Therapies and Sense of Purpose
Vaccine, nivolomab combination appears promising in recurrent HPV-related cancer
Treatment with a novel, synthetic, long-peptide HPV-16 vaccine plus nivolumab yielded promising response rates and survival outcomes among a small cohort of patients with incurable HPV-16-positive cancer, according to results from a single-arm phase 2 study.
The combination of the vaccine and anti-PD-1 immune checkpoint antibody induced an overall response rate of 33% and median OS of 17.5 months.
“That encouraging response rate is about twice the rate produced by PD-1 checkpoint inhibitors in previous clinical trials, so these results will lead to larger, randomized clinical trials of this combination,” “Vaccines are revving up the immune system, but the immunosuppressive tumor microenvironment probably prevents them from working. Our thinking was that inhibition of PD-1 would address one mechanism of immunosuppression, empowering the vaccine-activated T lymphocytes to attack the cancer.”
The analysis included 24 patients (median age, 60 years; men, n = 20) with incurable HPV-16-related cancers (oropharyngeal, n = 22; cervical, n = 1; anal, n = 1).
Patients received 100 mcg/peptide ISA101 on days 1, 22 and 50, and 3 mg/kg nivolumab (Opdivo) every 2 weeks, beginning on day 8 for up to 1 year.
ORR per Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1 served as the primary endpoint.
Of the eight patients who initially responded to the combination for a median duration of 10.3 months, five remained in response at study cutoff.
Median PFS was 2.7 months (95% CI, 2.5-9.4) and median OS was 17.5 months (95% CI, 17.5 months to inestimable).
At 6 months, PFS was 37% (95% CI, 22-63) and OS was 75% (95% CI, 59-94). At 1 year, PFS was 25% (95% CI, 12-50) and OS was 70% (95% CI, 54-91).
Researchers observed a grade 3 transaminase level elevation in one patient, and grade 4 lipase elevation in another, which led to discontinuation of nivolumab.
“The results of our trial are among the first clinical data to support the general concept of combining cancer vaccination with immune checkpoint blockade to enhance efficacy of vaccine-activated T cells in the immunosuppressive tumor environment,” the researchers wrote. “A randomized clinical trial testing the contribution of ISA101 to PD-1 inhibition in patients with platin-resistant HPV-16-positive recurrent oropharyngeal cancer is planned.” – by Jennifer Southall
Disclosures: The study was supported by Abell-Hangar Foundation Chair, University of Texas MD Anderson Cancer Center HPV-Related Cancers MoonShot, University of Texas MD Anderson Cancer Center Oropharynx Program Stiefel Gift, and University of Texas MD Anderson Cancer Center Support Grant P30CA016672. Bristol-Myers Squibb and ISA Pharmaceuticals approved the design of the study and reviewed the data presented. Glisson reports no relevant financial disclosures. Please see the study for all other authors’ relevant financial disclosures.