

Recently Diagnosed or Relapsed? Stop Looking For a Miracle Cure, and Use Evidence-Based Therapies To Enhance Your Treatment and Prolong Your Remission
Multiple Myeloma an incurable disease, but I have spent the last 25 years in remission using a blend of conventional oncology and evidence-based nutrition, supplementation, and lifestyle therapies from peer-reviewed studies that your oncologist probably hasn't told you about.
Click the orange button to the right to learn more about what you can start doing today.
- You are here:
- Home »
- Blog »
- Multiple Myeloma »
- Will the Multiple Myeloma Cancer Coaching Program Help Me?
Will the Multiple Myeloma Cancer Coaching Program Help Me?


Should we treat patients with myeloma with multidrug, multitransplant combinations with the goal of potentially curing a subset of patients, recognizing that the risk of adverse events and effect on quality of life will be substantial?
Hi David- My wife was diagnosed with Multiple Myeloma in March 2020 and entered (VDT) induction treatment in April. She had a successful stem cell harvest yesterday and is scheduled for a stem cell transplant in November. Do you feel The MM CC Program (Multiple Myeloma Cancer Coaching) would help me and, therefore, my wife? Don
Hi Don- I am sorry to learn of your wife’s MM diagnosis. The answers to your questions depend on certain specifics about your wife’s situation.
- How old is your wife?
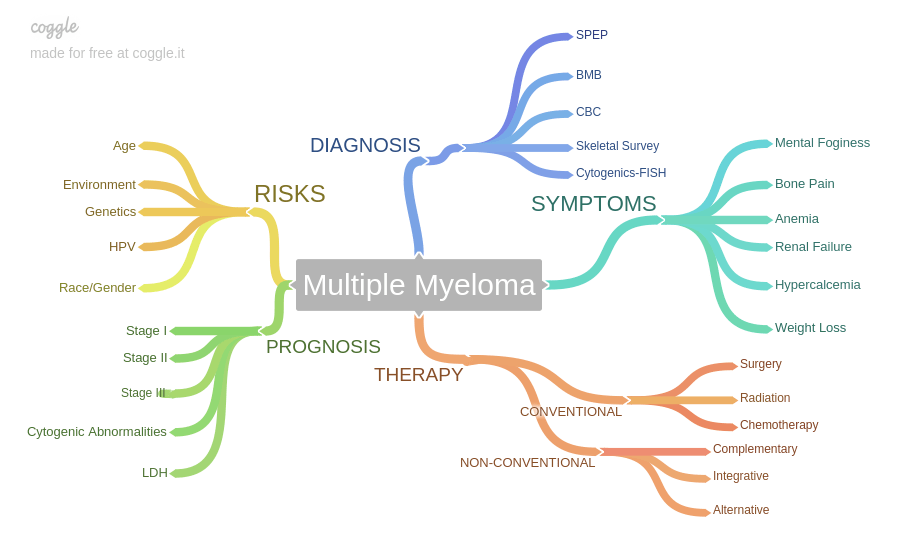
- What was your wife’s stage at diagnosis? If you weren’t given a stage, what were her symptoms? Bone, kidney health? M-spike, freelight chain, immunoglobulins? Any genetic abnormalities?
- What was her response to her induction chemotherapy? Complete response, very good partial response, partial response, etc.
I ask these questions because her prognosis will range greatly depending- for example, if she is 45 yrs, early stage, no genetic abnormalities, deep response to induction, then her prognosis will be 8-12 years. You will be able to guide her well as her knowledgeable caregiver. However, if she is 65 yrs, stage 2 or 3, bone or kidney involvement, with only a partial response, etc. then her prognosis is 2-5 years and you may have your hands full guiding her.
I’m biased of course, but I think MM is a difficult enough blood cancer that your wife will need both the guidance of a knowledgeable caregiver as well as the MM CC program (multiple myeloma cancer coaching program).
Let me know, thanks.
David Emerson
Reply to your questions-
1. How old is she?
Dotty is sixty and very fit (she doesn’t drink and is into swimming and long distance hiking).
She has IgA lambda Myeloma. This was an incidental discovery via a routine blood test in June 2019, which revealed Dot was somewhere between MGUS and Smouldering Myeloma.
2. What was her stage at diagnosis? If you weren’t given a stage, what were her symptoms? Bone, kidney health? M-spike, freelight chain, immunoglobulins? Any genetic abnormalities?
She was given no stage, but a full body MRI revealed a few small ( <5mm) lytic lesions in some of her bones. She has been on bisphosphonate infusions to stabilse these. She has some hip pain, but has needed no strong painkillers. Moreover, she has been a marathon runner and had a triple ankle fracture 5 years ago, so the lower half of her skeleton carries some wear and tear.
All major organs, including kidneys, are in perfect shape. Her lambda free light chain was 930 at the start of her induction; it is now at the normal level. Her paraproteins were at 70 at the start of her treatment (is this the same as ‘M-spike’?) She had around 60%* clonal plasma cells in her bone marrow just before the start of her treatment. That marrow sample was analysed and found to feature no genetic abnormalities.
3. What was her response to her induction chemotherapy? Complete response, very good partial response, partial response, etc
Dotty had a VGPR to her induction. Her most recent blood test, taken after 19 of her 20 Velcade shots, recorded her paraprotein as “Just detectable via immunofixation” (quote from pathology lab). She has withstood the treatment (5 cycles of VDT) very well.
*Dot went from 17% in her first bone marrow sample in August 2019 , to 60% in March 2020. Her MM appears to be aggressive. Dotty’s excellent Haematologist didn’t want to go for treatment so soon, but Dot had moved from Smouldering Myeloma to full-blown MM in seven months, so she made the call to start her on induction straight after the March 2020 marrow biopsy.
Dot is uneasy about HSCT, but her Haematogist is of the view that without it Dot will probably need to be back into VDT or something similar in 12 months’ time. It’s not great, but Dot is eating well, she has a positive mindset and practices meditation every day.
She is not frightened of death, and has barely shed one tear since receiving her diagnosis so we have been obliged to look the Grim Reaper straight in the eye.
Don- Several issues for you to consider.
First and foremost, according to research (see the study below), Dot’s overall survival (OS- length of life) will be the same regardless if she has an autologous stem cell transplant sooner or later. In other words, because Dot responded well to her induction therapy, a VGPR, studies show no difference between having an ASCT now or later.
If Dotty is reluctant to have an ASCT in any way, you both can see how the next year unfolds before making a decision. BTW, having harvested stem cells already insures the possibility of an ASCT whether Dot has one or not.
Secondly, Dotty’s age, stage, attitude, lifestyle and response to her induction therapy put her in a good position for both an ASCT and low-dose maintenance chemotherapy.
By this I mean that it is probable that your oncologist will talk up an ASCT followed by maintenance therapy in an effort to achieve a “deep remission” and a long overall survival. While the odds are in favor of Dot’s achieving a deep remission, a long progression-free survival (PFS- first remission) and therefore a longer than average life expectancy, the best case scenario if you go the conventional “standard-of-care” route is a 10-20 year length of life.
I believe that Dotty will live a higher quality of life and a longer quantity of life by undergoing low doses of chemo combined with anti-MM nutrition, supplementation, lifestyle, etc.
This approach is the answer to your questions and what the MM CC Program focuses on. Basically following conventional oncology or following the MM CC Program by combining conventional therapies with non-conventional therapies.
Please read the Cure vs. Control article linked below. Conventional oncology is the “cure” approach and I am the “control” approach.
Finally, research shows that involved caregiving results in longer OS for MM patients. Deb will benefit either way with your involvment.
Let me know if you have any questions.
David Emerson
- MM Survivor
- MM Cancer Coach
- Director PeopleBeatingCancer
Recommended Reading:
Multiple Myeloma Response-CR or VGPR- NO Difference
“It would be logical to think that a CR or VGPR status translated into a longer overall survival. I know I thought this when I had my autologous stem cell transplant. According to the two studies linked and excerpted below, I was wrong to think this.
To Enlarge, Click the image below-
Please don’t misunderstand me. Yes, a CR is a positive indicator for a longer overall survival. But the opposite is not true. Not achieving a CR does not mean that you will not live a long OS…”
Treatment of Myeloma: Cure vs Control
“Although not often openly acknowledged, “cure vs control” is the dominant philosophical difference behind many of the strategies, trials, and debates related to the management of myeloma. Should we treat patients with myeloma with multidrug, multitransplant combinations with the goal of potentially curing a subset of patients, recognizing that the risk of adverse events and effect on quality of life will be substantial? Or should we address myeloma as a chronic incurable condition with the goal of disease control, using the least toxic regimens, emphasizing a balance between efficacy and quality of life, and reserving more aggressive therapy for later?…”