

Recently Diagnosed or Relapsed? Stop Looking For a Miracle Cure, and Use Evidence-Based Therapies To Enhance Your Treatment and Prolong Your Remission
Multiple Myeloma an incurable disease, but I have spent the last 25 years in remission using a blend of conventional oncology and evidence-based nutrition, supplementation, and lifestyle therapies from peer-reviewed studies that your oncologist probably hasn't told you about.
Click the orange button to the right to learn more about what you can start doing today.
- You are here:
- Home »
- Blog »
- Multiple Myeloma »
- Multiple Myeloma Chemotherapy-VCD-Lite, RVD-Lite
Multiple Myeloma Chemotherapy-VCD-Lite, RVD-Lite


““The best regimens maximize the likelihood of multiple myeloma control, ie, efficacy, while minimizing risk of severe toxicity…”
You’ve been diagnosed with an incurable blood cancer. You’ve probably never heard of this type of cancer. You have to rely on your oncologist to prescribe the multiple myeloma chemotherapy that is right for you. But what does “right for you” mean?
Consider the experience of a long-term MM survivor who has worked with hundreds of MM patients since 2005.
If you could undergo a well-researched multiple myeloma chemotherapy cocktail (triplet) that has been the standard-of-care for thousands of previous newly diagnosed MM patients, undergoing that MM combo would make sense to you, right?
Now consider if that same chemotherapy combo was given to at a lower dose. Lower dose means less chemotherapy which means less toxicity. Less toxicity means less damage to your body.
The studies linked below proved the triplet resulted in fewer short, long term and late stage side effects.
Both multiple myeloma chemotherapy cocktails discussed in the research below RVd (revlimid, velcade, dexamethasone) and VCd (velcade, cyclophosphamide, dexamethasone) are extremely effective at stabilizing MM patients. Both regimens are known to have a high overall response rate. That statistic simply means that a high percentage of people “responded.”
The difference between the full RVd and VCd and RVd lite and VCd lite is that the doses of each chemotherapy are reduced.
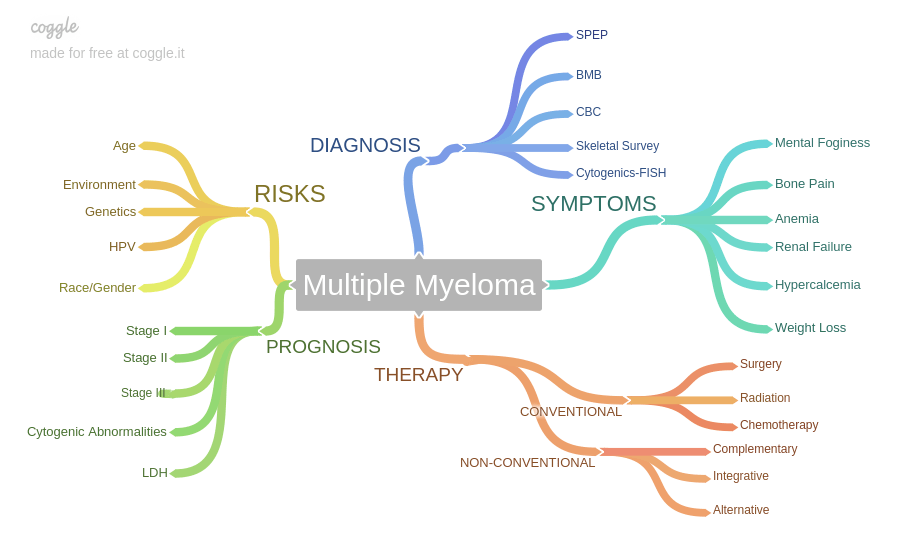
What is Multiple Myeloma? Oncology has it backwards…
The point of the blog post linked above is that the most common MM symptoms are the most common side effects which also happen to be the most common causes of death for multiple myeloma survivors.
Myeloma causes immune, bone, kidney and heart damage while toxic chemotherapy regimens also cause immune, bone, kidney and heart damage.
Less chemotherapy means less toxicity which result in less organ damage. Consider RVd lite. Less is more.
Have you been diagnosed with multiple myeloma? What stage? What symptoms are you experiencing? To learn more about evidence-based, non-toxic therapies shown to fight MM while they heal bones and heal kidneys scroll down the page, post a question or comment and I will reply to you ASAP.
Thank you,
David Emerson
- MM Survivor
- MM Cancer Coach
- Director PeopleBeatingCancer
Recommended Reading:
- Multiple Myeloma Chemotherapy = Accelerated Aging
- Multiple Myeloma Induction- RVD W/ or W/O ASCT?
- Multiple Myeloma- Black Seed Oil, TQ- Kill MM, Pro Bone, Kidney, Heart-
Updated Results of a Phase 2 Study of Modified Lenalidomide, Bortezomib, and Dexamethasone (RVd-lite) in Transplant-Ineligible Multiple Myeloma
“RVD lite was administered over a 35-day cycle. Lenalidomide 15 mg was given orally days 1-21; bortezomib 1.3 mg/m2 once weekly subcutaneously (SC) on days 1, 8, 15, and 22; dexamethasone 20 mg orally day of and after bortezomib for 9 cycles followed by 6 cycles of consolidation…
Primary objective was to evaluate overall response rate (ORR). Secondary objectives included evaluation of safety, progression free survival (PFS), overall survival (OS), and the pharmacokinetic (PK) profile of intravenous (IV) and SC bortezomib…
Fatigue was the most commonly reported toxicity occurring in 37 (74%) and was mostly grade 1 or 2 in 29 (58%).
Other grade 3 or greater toxicities included:
- hypophosphatemia in 17 (34%),
- neutropenia in 7 (14%), and
- rash in 5 (10%) pts.
Low grade peripheral neuropathy was reported in 31 (62%) patients with only 1 patient experiencing grade 3 symptoms…
The ORR was 86% and 66% of patients achieved a very good partial response (VGPR) or better. The median time to response was 1.1 months. At a follow-up of 61 months, median PFS was 41.9 months (95% CI, 31.2 – ∞) and median OS not reached. The 5-year overall survival was 61.3%. Sixty-six percent of patients received lenalidomide maintenance…
VCD-Lite’ Viable Option for Older, Toxicity-Vulnerable Myeloma Patients
“Dose-attenuated bortezomib, cyclophosphamide, and dexamethasone (VCD-lite) is a viable treatment option for vulnerable or frail adults with newly diagnosed multiple myeloma, according to the results of a small study published in the Journal of Geriatric Oncology…
“The best regimens maximize the likelihood of multiple myeloma control, ie, efficacy, while minimizing risk of severe toxicity. This is of particular importance in the vulnerable patient population under discussion, which is especially subject to severe sequelae of toxicity due to the loss of homeostatic reserve that arises with normal aging, compounded in many cases by specific medical comorbidities…”
According to the study, undergoing full-dose chemotherapy with VCD often leads to excessive toxicity in very old or frail adults with newly diagnosed multiple myeloma…
Sixty-four percent of patients experienced grade 3 or worse adverse events; 14% of patients discontinued treatment due to toxicity, 26% due to progression, and 29% due to other reasons…