

Diagnosed with Cancer? Your two greatest challenges are understanding cancer and understanding possible side effects from chemo and radiation. Knowledge is Power!
Learn about conventional, complementary, and integrative therapies.
Dealing with treatment side effects? Learn about evidence-based therapies to alleviate your symptoms.
Click the orange button to the right to learn more.
- You are here:
- Home »
- Blog »
- side effects ID and prevention »
- Late Progressive Anthracycline – What’s in Store for Me?
Late Progressive Anthracycline – What’s in Store for Me?


“Late onset arrhythmia and sudden death has occurred more than 15 years after anthracycline treatment [8].” Sudden death??? Yikes!
Anytime I read the words “sudden death,” particularly when it applies to me, I freak. You see, I underwent six courses of a chemo-cocktail called V.A.D. (anthracycline chemotherapy), then I underwent two courses of high-dose cyclophosphomide and then busulphan and melphalan all throughout 1995. I experienced an odd echo test while in treatment but since my cardiologist said that my reduced ejection fraction was “within normal limits” and that I had nothing to worry about, I figured I was fine.
In hindsight, that reduced EJ should have tipped off my cardiologist that the 6 rounds of VAD, cytoxan, busulfan and melphalan was causing short, long-term and late stage problems for me.
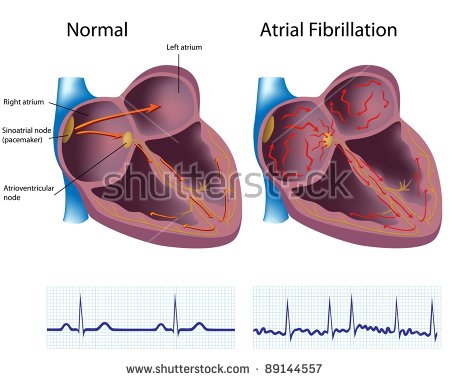
I developed chronic atrial fibrillation 15 years later in late 2010 and was diagnosed with chemotherapy-induced cardiomyopathy in early 2019. So the article linked below is describing me to a tee.
What bothers me most about the article below is that it states that “Anthracycline-induced cardiotoxicity has been recognized for more than 20 years.” That statement was written in 2009. According to the article then, my oncologist AND my cardiologist should have known that Anthracycline-induced cardiotoxicity could be a problem for me.
More to the point, because the cardiotoxicity experienced by the cancer patient (me) is dependant on the accumulated dose AND the accompanying therapies, I was almost guaranteed to experience heart damage.
If you’re wondering, no, all of my aggressive, cardiotoxic therapies did not kill my cancer. After two short remissions I was told that “nothing more could be done for me.”
Did you recieve anthracyclines chemotherapy at any point during your active cancer therapy? To learn more about evidence-based therapies shown to enhance heart health, scroll down the page, post a question or comment and I will reply to you ASAP.
Thank you,
David Emerson
- Cancer Survivor
- Cancer Coach
- Director PeopleBeatingCancer
Recommended Reading:
Chemotherapy Induced Cardiomyopathy: Pathogenesis, Monitoring and Management
“Cardiotoxicity may depend on the dose administered during each course or on the total cumulative dose, or may be completely independent of the dose like Anthracycline-induced cardiotoxicity which has been recognized for more than 20 years. It has been described as 3 distinct types of cardiotoxicity…
Late onset chronic progressive anthracycline cardiotoxicity causes ventricular dysfunction [5], heart failure and arrhythmias [6] years to decades after chemotherapy has been completed.
This suggests that patients who have received anthracyclines chemotherapy and survived their cancer may have undetected increases in morbidity and mortality due to cardiotoxicity. There may be a period of time, after completion of treatment, during which patients may experience no symptoms of left ventricular dysfunction or arrhythmia and cardiac function may appear normal.
After the initial acute myocardial insult, there is a progressive decrease in ventricular function leading to late onset decompensation. An increased incidence of severe echocardiographic abnormalities has been seen with increased duration of follow-up.
An 18% incidence of reduction in fractional shortening on resting echocardiogram was observed 4 to 10 years after completion of anthracycline therapy [6]. Cumulative doses of doxorubicin as low as 228 mg/m2 have shown to increase after-load or decrease contractility, or both, in 65% of patients with leukaemia up to 15 years after treatment with anthracyclines [7].
Late onset arrhythmia and sudden death has occurred more than 15 years after anthracycline treatment [8]. This could mean that more anthracyclines induced cardiotoxicity may appear in the future in patients who are presently asymptomatic. Patients may remain in a compensated state for many years until stressors such as acute viral infection [9] or cardiovascular stressors such as weight lifting, pregnancy and surgery [6] could possibly trigger a cardiac event…
Risk factors for cardiotoxicity
Some of the risk factors relating to early and late (but not acute) cardiotoxicity have been reported. These include:
- cumulative dose,
- rate of drug administration,
- mediastinal radiation,
- advanced age,
- younger age,
- female gender,
- pre-existing heart disease and
- hypertension.
A multivariate analysis of these factors based on histological evidence of anthracycline-induced cardiac damage concluded that higher rates of administration and previous cardiac irradiation were independent risk factors. At a cumulative total dose of < 400 mg/m2 body surface area, the incidence of CHF was found to be 0.14%. This increased to 7% at a dose of 550 mg/m2 and to 18% at a dose of 700 mg/m2 [4].
There is a formula to calculate the cardiac toxicity as follow Y= (X)2/a, Y is the likelihood of developing congestive heart failure, X equals to number of cycles of anthracycline-containg regimen administered, a equals to correction constant determined by cycle dose and the duration between the cycles, so if a patient receives 9 cycle of anthracycline in a dose of 50 mg/m2 every 21 days, so it will be Y= 81/16 X100, the Y will be equal to 5%, this is the risk of developing congestive heart failure [4]…
Physical examination alone may miss over 50% of cases of early and reversible chemotherapy-induced CHF [12]. Acute ECG changes and arrhythmias following doxorubicin therapy occur in 0 to 14% of patients. Serial measurements of LVEF and fractional shortening are the most common indices monitored to assess left ventricular systolic function and cardiotoxicity…
This can be achieved by 2-dimensional, M-mode and color Doppler echocardiographic examination. Baseline LVEF estimation is recommended before the start of doxorubicin therapy. If LVEF is ≤ 30%, starting chemotherapy is not recommended. Patients with LVEF ≥ 30% but <50% can receive doxorubicin, but measurements should be repeated before each dose. For patients with baseline LVEF ≥ 50%, evaluations should be repeated after a cumulative dose of 250 to 300 mg/m2 and thereafter at 450 mg/m2 if they have no risk factors. If patients have known cardiovascular disease, prior radiation treatment to the chest, abnormal ECG changes or concomitant cardiotoxic chemotherapy, LVEF measurement should be repeated at 400 mg/m2 instead of 450 mg/m2. It should be monitored with each dose thereafter. Doxorubicin therapy should be stopped if there is a ≥ 10% absolute drop in the ejection fraction associated with a decrease in LVEF to ≤ 50% in patients with baseline LVEF ≥ 50%, and to ≤ 30% in patients with baseline LVEF < 50% but > 30% [13]…
At the end, frequent monitoring and follow up for patients took anthracyclines with troponins and echocardiograms with early administration of carvedilol, enalapril and probably with anti-oxidants like Probucol and vitamin E will benefit.”