

Diagnosed with SMM, SPB, or MGUS?
Learn how you can stall the development of full-blown Multiple Myeloma with evidence-based nutritional and supplementation therapies.
Click the orange button to the right to learn more.
- You are here:
- Home »
- Blog »
- Multiple Myeloma »
- It’s Either Smoldering Multiple Myeloma or Multiple Myeloma
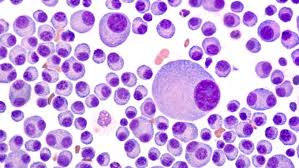
It’s Either Smoldering Multiple Myeloma or Multiple Myeloma


If you are not young, early stage (MM) and low-risk then, according to the research below, your average first remission will be about 2-3 years and your OS will be about the average 5-7 years.
Hi David- Thank you for sharing this! I am currently awaiting diagnosis, but it’s either Smoldering Multiple Myeloma or MM. I am grateful to have found your site with all the nutritional and lifestyle recommendations. Will be working on integrating them into my diet and lifestyle.
I had been working toward adopting the Budwig diet, but found it very limiting (and a lot of work to keep up with). I am glad to know I that I don’t have to go whole hog on that one! Lisa-
Hi Lisa-
- Do you know your m-spike?
- Do you have any CRAB symptoms such as bone pain, kidney damage?
- Do you know your immunoglobulin and/or freelight chain levels?
I don’t mean to sound nosey. Just wondering.

If you are diagnosed as smoldering multiple myeloma you don’t have cancer, you have a “blood disorder” according to conventional oncology. While conventional oncology does not offer therapy for SMM, consider the many non-conventional therapies shown to reduce the risk of multiple myeloma.
- Anti-angiogenic nutrition (Budwig protocol)-
- Anti-angiogenic nutritional supplementation-
- Detox. therapies-
- Lifestyle therapies-
- Others-
If you are diagnosed with frank multiple myeloma, you are early stage. There are several documented benefits to early stage MM. 95% of MM diagnoses are stage 2 or 3 so early stage MM is relatively rare.
All of the non-toxic, anti-MM therapies that you undergo now, before you undergo conventional therapies is considered to be “pre-habilitation.” Pre-habilitating, according to research, will help you respond better to therapy if and when you do it, and help you heal faster after conventional therapies. I will link studies documenting pre-habilitation’s benefits below.
Further, early stage MM is almost a different disease than MM stage 2 or stage 3. By this I mean that, in my opinion, the standard-of-care MM therapy plan is too much toxicity for you.
The SOC for MM is
- Induction chemotherapy (RVD)
- Autologous Stem Cell Transplant
- Maintenance chemotherapy-
Too much toxicity that can cause short, long-term and late stage side effects. Too much toxicity that will speed you toward multi-drug resistance MDR.
I will link a post I wrote about the best case/worst case scenario approach to ASCT.
Please consider consulting with Dr. James Berenson. Dr. Berenson is the only MM specialist I know of who takes a low-dose, low-toxicity approach to managing MM. Dr. Berenson has the longest/best five year MM survival rates in the world.
If you don’t live in CA, you can consult with Dr. Berenson. Your local oncologist can prescribe any FDA therapies or order any diagnostic tests.
http://www.berensononcology.com
My point is that you have many options being either pre-MM or early stage MM.
Let me know if you have any questions.
Hang in there,
David Emerson
- MM Survivor
- MM Cancer Coach
- Director PeopleBeatingCancer
Recommended Reading:
- Multiple Myeloma Cancer Coaching Q & A
- MGUS (pre-myeloma) and Kidney Damage
- Cancer Coaching Testimonials- PeopleBeatingCancer
Beating Myeloma: “If I Knew Then What I Know Now”
- young as MM patients go
- early stage MM (stage 1)
- low risk (no genetic abnormalities)
If you are not young, early stage and low-risk then, according to the research below, your average first remission will be about 2-3 years and your OS will be about the average 5-7 years.
But there is a better way…
To make matters worse, according to the second study linked and excerpted below, if you do achieve a long progression-free survival (PFS) and a long overall survival (OS) you stand a good chance of living with short, long-term and late stage side effects. Specifically:
- endocrinopathies,
- musculoskeletal disorders,
- cardiopulmonary compromise and
- subsequent malignancies.
According to the study, you will live in debilitating pain for the rest of your life.
But there is a better way…
My point in telling you all this is not to be gruesome and depressing. There is another way.
My point is to explain what is called the “standard-of-care” for NDMM patients. Basically, the SOC for average MM patients is much too much chemotherapy, way too much toxicity in my experience.
Yet, board-certified oncologists, as intelligent and well-trained as they are, must prescribe what the Food and Drug Administration has approved as the SOC. This is how the FDA chooses to standardize MM treatment. This is how medicine works in the United States.
Chemotherapy may be necessary to stabilize your MM. But you may not need as much chemotherapy as the SOC prescribes- induction chemo regimen (RVD), an autologous stem cell transplant (ASCT) and maintenance therapy.
Cancer prehabilitation: One step toward improved outcomes
“Prehabilitation is not a new concept, nor is it specific to cancer. At its core, prehabilitation is designed to improve a person’s physical and psychological health in anticipation of an upcoming stressor. Furthermore, prehabilitation is part of the rehabilitation care continuum and is defined temporally as those assessments and interventions that occur after diagnosis but before acute treatment begins…
Many of the early studies on cancer prehabilitation typically focused exclusively on building strength and stamina through an appropriate exercise regimen; however, more recent research has supported a multimodal approach that encompasses more than one intervention (ie, a combination of exercise, nutrition, and psychological strategies) to better prepare patients for the challenges associated with upcoming cancer treatments.2…”